Microvascular decompression (MVD) is a surgical procedure for relieving pressure on the trigeminal nerve caused by offending blood vessel, done by placing cushion between the two and is considered highly effective treatment for trigeminal neuralgia (TN). DFP refer to the facial paralysis which occurs more than 24 hours after MVD procedure and it can generally recover spontaneously. It common in clinical observation and its mechanism is still unclear. Facial paralysis can result from several mechanisms which includes inadvertent injury to the facial nerve as during the MVD surgery, the facial nerve, which lies in close proximity to the trigeminal nerve, can be at risk. Even a small amount of trauma to the facial nerve can lead to temporary or permanent weakness. Post-surgical swelling or inflammation: Following MVD, the surrounding tissues, including the facial nerve, can experience swelling or inflammation. This may temporarily impair the function of the facial nerve. Anatomical variations: Variations in the anatomy of the vascular structures or the proximity of the facial nerve can increase the likelihood of facial nerve involvement during decompression. The management of post-operative facial paralysis typically involves a thorough evaluation to determine whether the condition is transient (due to inflammation or mild injury) or more persistent, which might require further intervention. Conservative treatments, such as corticosteroids or physical therapy, are often recommended for mild cases, while more severe or persistent cases might necessitate additional surgical approaches.
This is an Open Access article, distributed under the terms of the Creative Commons Attribution 4.0 International License (http://creativecommons.org/licenses/by/4.0/), which permits unrestricted use, distribution and reproduction in any medium or format, provided the original work is properly cited.
MVD, TN, V2, V3, SCA, Superior Cerebellar Artery, Microvascular Decompression, DFP, Delayed Facial Paralysis, Trigeminal Neuralgia, Vascular Compression, Surgery
1. Introduction
We present one such case of a young female presenting with left sided facial pain with V2, V3 distribution from 4 months, case illustrates a common clinical scenario where MVD offers significant relief for TN, particularly when the radiological findings shows a loop of the superior cerebellar artery (SCA) abutting the trigeminal nerve confirming vascular compression. The development of facial paralysis in the follow-up period, though rare, is a potential complication of MVD, and it highlights the complexities of the procedure.
2. Case 1
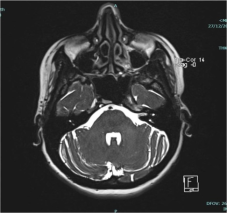
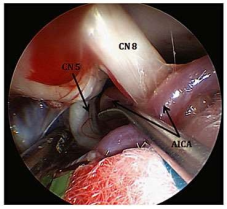
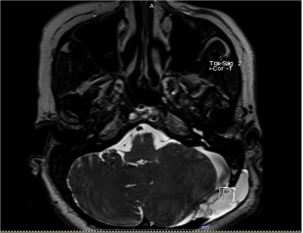
A 44-year-old woman with a history of hypertension and a chief complaint of left-sided facial pain in the V2 and V3 distributions, which had been ongoing for 4 months. MRI of the brain with trigeminal protocol revealed that the left superior cerebellar artery (SCA) was in close contact with the cisternal segment of the left trigeminal nerve near its root entry zone, indicating a potential cause for trigeminal neuralgia. (Figure 1) She underwent microvascular decompression (MVD) surgery, a common procedure used to relieve trigeminal neuralgia. Offending vascular structure was seperated from the trigeminal nerve via a teflon patch.res from the trigeminal nerve, which led to resolution of her facial pain. (Figure 2). Patient was discharged. She was discharged on tapering dose of neuropathic medication.
Figure 1. MRI of the brain with trigeminal protocol revealed that the left superior cerebellar artery (SCA) was in close contact with the cisternal segment of the left trigeminal nerve near its root entry zone.
Figure 2. Teflon patch placed separating trigeminal nerve from loop of superior cerebellar artery.
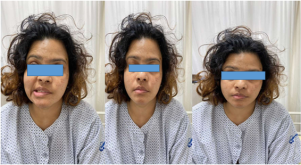
However, during follow-up, the patient develop grade 2 facial paralysis characterised by slight facial weakness, normal symmetry at rest and complete eye closure with minimal efforts.
2.1. Follow up Period After 2 Week
Patient presenting with grade II facial paresis and mild imbalance while walking.
Facial paralysis following microvascular decompression can occur due to a few possible reasons:
1) Direct Injury to the Facial Nerve: The facial nerve (cranial nerve VII) runs in close proximity to the trigeminal nerve in the brainstem and may be inadvertently injured during the surgical procedure, especially if the decompression requires manipulation of surrounding structures.
2) Trauma from Retraction: In some cases, retraction of the cerebellum or the brainstem during surgery may cause mechanical injury to the facial nerve.
3) Post-operative Edema or Compression: After MVD, post-operative swelling or hematoma can put pressure on the facial nerve, leading to temporary or permanent paralysis.
4) Ischemia or Vascular Compromise: There is also a risk of ischemia to the facial nerve if blood flow is disrupted during the surgery, although this is less common.
5) Pre-existing Subclinical Facial Nerve Dysfunction: In some cases, a prior undiagnosed issue with the facial nerve (such as minor compression or preexisting vulnerability) may become symptomatic postoperatively.
Figure 5. Post operative MRI showing inflammatory changes around facial nerve.
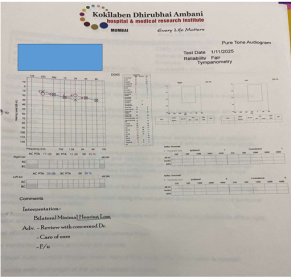
Repeat MRI done shows pseudomenigocele and inflammatory changes around facial nerve. Patient was started on high dose steroid there was gradual improvement in the facial weakness and gait. Pure tone audiometry showed bilateral minimal hearing loss. No retraction injury to auditory nerve.
3. Discussion
MVD has remained the gold standard surgery for the treatment of TN and HS, providing excellent long term results. The most common complications include CSF leak, facial hypoesthesia, facial paresis, chemical meningitis and hearing loss. Delayed facial weakness is an uncommon complication, mostly reported after MVD for HS. The incidence of DFP following MVD for hemifacial spasm have been reported about 2.5-8.3%. DFP following MVD for TN is rare only few cases have been reported in literature Average time for onset of DFP after surgery ranges from1week to12 days,
DFP patients did not show immediate facial paralysis after operation indicating that decompression does not damage the nerve. The etiology of DFP remains unclear. Long term compression of facial nerve root by the responsible blood vessel may lead to demyelinating lesion which result in the facial nerve root more sensitive to the mechanical injury during the operation or heterogeneous stimulation of decompression pad cotton and subsequently leading to the delayed edema.
[11]
Maarbjerg S, Di Stefano G, Bendtsen L, Cruccu G. Trigeminal neuralgia - diagnosis and treatment. Cephalalgia. 2017 Jun; 37(7): 648-657.
[11]
Kim et al opined that the possible causes include facial nerve exit zone injury through the Teflon patch or delayed facial nerve edema. Early occurrence of DFP was mainly due to mechanical injury during operation and subsequent nerve root edema while late occurrence of DFP was due to heterogeneous stimulation of Teflon patch can cause long term allergic reaction where edema subsides slowly
[8]
KIM, B.-T. et al. Delayed facial palsy following microvascular decompression in hemifacial spasm patients. J. Korean Neurosurg. Soc. 1332–1336 (1999).
Hence, they instituted postoperative vasoactive therapy with nimodipine for patients with DFP after acoustic neuroma surgery and noted that all their patients improved. Neural edema has been proposed as a cause of DFP. It mainly occurs at the level of the meatal foramen and plays a deleterious role at the fundus of the meatus because this is the narrowest part of the Fallopian canal. Liu et al. concluded that hypertension might be a contributing factor for occurrence of DFP as noted in their series of 16 DFP cases.
[10]
Liu L X, Zhang C W, Ren P W, et al. Microvascular decompression for trigeminal neuralgia: Recurrences and complications. J Clin Neurosci. 2005; 12(7): 787-789.
Small hemorrhages into the facial canal and partial neural necrosis may explain the association between hypertension and facial palsy. A possible viral etiology in the form of reactivation of herpes simplex virus (HSV) or varicell a zoster virus as a cause of DFP has been proposed by many authors. Gianoli has pointed out that DFP is closely related to the increased IgM titers of herpes simplex virus (HSV) and varicella zoster virus (VZV). HSV and VZV can hide in the ganglion to avoid the interference of antibody and be usually dormant in the geniculate ganglia. Operation may be a stimulating factor to activate the virus resided in the geniculate ganglia. Activation of virus is a gradual process, and finally causes DFP. The increased titers of HSV antibodies have been reported in some DFP patients. It is crucial to thoroughly evaluate and monitor post-surgical conditions. Delayed facial weakness in this case may be attributed to gradual edema occurring after surgery. The use of Teflon to separate nerve tissue and blood vessels, although beneficial, can sometimes be perceived as a foreign body leading to inflammation.
[1]
Günther, T. et al. Microvascular decompression for trigeminal neuralgia in the elderly: long-term treatment outcome and comparison with younger patients. Neurosurgery 65, 477–482 (2009).
Han, J.-S., Lee, J.-A., Kong, D.-S. & Park, K. Delayed cranial nerve palsy after microvascular decompression for hemifacial spasm. J. Korean Neurosurg. Soc. 52, 288 (2012).
Prasad, G. L., Kumar, V. & Menon, G. Delayed facial palsy after microvascular decompression: report of two cases. J. Neurosci. Rural Pract. 8, 461–465 (2017).
Guthikonda, B., Pensak, M. L. & Theodosopoulos, P. V. Delayed facial palsy after the anterior petrosal approach: case report and review of the literature. Neurosurgery 66, E845–E846 (2010).
[7]
Rhee, D. J., Kong, D. S., Park, K. & Lee, J. A. Frequency and prognosis of delayed facial palsy after microvascular decompression for hemifacial spasm. Acta Neurochir. (Wien). 148, 839–843 (2006).
Several treatments have been proposed to address DFP including steroids, acyclovir, and facial canal decompression. But in most cases spontaneous resolution occurs, and the average duration of improvement is 5.7-9 weeks.
[8]
KIM, B.-T. et al. Delayed facial palsy following microvascular decompression in hemifacial spasm patients. J. Korean Neurosurg. Soc. 1332–1336 (1999).
Delayed facial paralysis after Microvascular Decompression (MVD) is a rare but serious complication. If a patient experiences delayed facial paralysis after MVD, it's important to undergo a thorough evaluation to determine the exact cause. This may involve MRI scans or CT scans to check for nerve compression, vascular anomalies, or other issues.
Electromyography (EMG) to assess the function of the facial nerve and muscles. Consultation with a neurologist or neurosurgeon to assess the cause and create an appropriate treatment plan. Treatment may include medications for inflammation or nerve recovery, physical therapy to improve facial muscle control, or, in rare cases, additional surgery. While delayed facial paralysis after MVD is rare, it is important to monitor for symptoms and consult a healthcare provider promptly if such symptoms occur. Early diagnosis and treatment are key to improving the chances of recovery.
Abbreviations
CSF
Cerebrospinal Fluid
DFP
Delayed Facial Spasm
HS
Hemifacial Spasm
HSV
Herpes Simplex Virus
MRI
Magnetic Resonance Imaging
MVD
Microvascular Decompression
PTA
Pure Tone Audiometry
SCA
Superior Cerebellar Artery
TN
Trigeminal Neuralgia
Conflicts of Interest
The author declares no conflicts of interest.
References
[1]
Günther, T. et al. Microvascular decompression for trigeminal neuralgia in the elderly: long-term treatment outcome and comparison with younger patients. Neurosurgery 65, 477–482 (2009).
Han, J.-S., Lee, J.-A., Kong, D.-S. & Park, K. Delayed cranial nerve palsy after microvascular decompression for hemifacial spasm. J. Korean Neurosurg. Soc. 52, 288 (2012).
Prasad, G. L., Kumar, V. & Menon, G. Delayed facial palsy after microvascular decompression: report of two cases. J. Neurosci. Rural Pract. 8, 461–465 (2017).
Guthikonda, B., Pensak, M. L. & Theodosopoulos, P. V. Delayed facial palsy after the anterior petrosal approach: case report and review of the literature. Neurosurgery 66, E845–E846 (2010).
[7]
Rhee, D. J., Kong, D. S., Park, K. & Lee, J. A. Frequency and prognosis of delayed facial palsy after microvascular decompression for hemifacial spasm. Acta Neurochir. (Wien). 148, 839–843 (2006).
Liu L X, Zhang C W, Ren P W, et al. Microvascular decompression for trigeminal neuralgia: Recurrences and complications. J Clin Neurosci. 2005; 12(7): 787-789.
Singh, P., Patel, H., Kumar, A. (2025). Rare Complication of Microvascular Decompression: Delayed Facial Paralysis. International Journal of Cardiovascular and Thoracic Surgery, 11(4), 41-44. https://doi.org/10.11648/j.ijcts.20251104.11
@article{10.11648/j.ijcts.20251104.11,
author = {Preeti Singh and Harsh Patel and Abhaya Kumar},
title = {Rare Complication of Microvascular Decompression: Delayed Facial Paralysis
},
journal = {International Journal of Cardiovascular and Thoracic Surgery},
volume = {11},
number = {4},
pages = {41-44},
doi = {10.11648/j.ijcts.20251104.11},
url = {https://doi.org/10.11648/j.ijcts.20251104.11},
eprint = {https://article.sciencepublishinggroup.com/pdf/10.11648.j.ijcts.20251104.11},
abstract = {Microvascular decompression (MVD) is a surgical procedure for relieving pressure on the trigeminal nerve caused by offending blood vessel, done by placing cushion between the two and is considered highly effective treatment for trigeminal neuralgia (TN). DFP refer to the facial paralysis which occurs more than 24 hours after MVD procedure and it can generally recover spontaneously. It common in clinical observation and its mechanism is still unclear. Facial paralysis can result from several mechanisms which includes inadvertent injury to the facial nerve as during the MVD surgery, the facial nerve, which lies in close proximity to the trigeminal nerve, can be at risk. Even a small amount of trauma to the facial nerve can lead to temporary or permanent weakness. Post-surgical swelling or inflammation: Following MVD, the surrounding tissues, including the facial nerve, can experience swelling or inflammation. This may temporarily impair the function of the facial nerve. Anatomical variations: Variations in the anatomy of the vascular structures or the proximity of the facial nerve can increase the likelihood of facial nerve involvement during decompression. The management of post-operative facial paralysis typically involves a thorough evaluation to determine whether the condition is transient (due to inflammation or mild injury) or more persistent, which might require further intervention. Conservative treatments, such as corticosteroids or physical therapy, are often recommended for mild cases, while more severe or persistent cases might necessitate additional surgical approaches.
},
year = {2025}
}
TY - JOUR
T1 - Rare Complication of Microvascular Decompression: Delayed Facial Paralysis
AU - Preeti Singh
AU - Harsh Patel
AU - Abhaya Kumar
Y1 - 2025/08/20
PY - 2025
N1 - https://doi.org/10.11648/j.ijcts.20251104.11
DO - 10.11648/j.ijcts.20251104.11
T2 - International Journal of Cardiovascular and Thoracic Surgery
JF - International Journal of Cardiovascular and Thoracic Surgery
JO - International Journal of Cardiovascular and Thoracic Surgery
SP - 41
EP - 44
PB - Science Publishing Group
SN - 2575-4882
UR - https://doi.org/10.11648/j.ijcts.20251104.11
AB - Microvascular decompression (MVD) is a surgical procedure for relieving pressure on the trigeminal nerve caused by offending blood vessel, done by placing cushion between the two and is considered highly effective treatment for trigeminal neuralgia (TN). DFP refer to the facial paralysis which occurs more than 24 hours after MVD procedure and it can generally recover spontaneously. It common in clinical observation and its mechanism is still unclear. Facial paralysis can result from several mechanisms which includes inadvertent injury to the facial nerve as during the MVD surgery, the facial nerve, which lies in close proximity to the trigeminal nerve, can be at risk. Even a small amount of trauma to the facial nerve can lead to temporary or permanent weakness. Post-surgical swelling or inflammation: Following MVD, the surrounding tissues, including the facial nerve, can experience swelling or inflammation. This may temporarily impair the function of the facial nerve. Anatomical variations: Variations in the anatomy of the vascular structures or the proximity of the facial nerve can increase the likelihood of facial nerve involvement during decompression. The management of post-operative facial paralysis typically involves a thorough evaluation to determine whether the condition is transient (due to inflammation or mild injury) or more persistent, which might require further intervention. Conservative treatments, such as corticosteroids or physical therapy, are often recommended for mild cases, while more severe or persistent cases might necessitate additional surgical approaches.
VL - 11
IS - 4
ER -
Singh, P., Patel, H., Kumar, A. (2025). Rare Complication of Microvascular Decompression: Delayed Facial Paralysis. International Journal of Cardiovascular and Thoracic Surgery, 11(4), 41-44. https://doi.org/10.11648/j.ijcts.20251104.11
@article{10.11648/j.ijcts.20251104.11,
author = {Preeti Singh and Harsh Patel and Abhaya Kumar},
title = {Rare Complication of Microvascular Decompression: Delayed Facial Paralysis
},
journal = {International Journal of Cardiovascular and Thoracic Surgery},
volume = {11},
number = {4},
pages = {41-44},
doi = {10.11648/j.ijcts.20251104.11},
url = {https://doi.org/10.11648/j.ijcts.20251104.11},
eprint = {https://article.sciencepublishinggroup.com/pdf/10.11648.j.ijcts.20251104.11},
abstract = {Microvascular decompression (MVD) is a surgical procedure for relieving pressure on the trigeminal nerve caused by offending blood vessel, done by placing cushion between the two and is considered highly effective treatment for trigeminal neuralgia (TN). DFP refer to the facial paralysis which occurs more than 24 hours after MVD procedure and it can generally recover spontaneously. It common in clinical observation and its mechanism is still unclear. Facial paralysis can result from several mechanisms which includes inadvertent injury to the facial nerve as during the MVD surgery, the facial nerve, which lies in close proximity to the trigeminal nerve, can be at risk. Even a small amount of trauma to the facial nerve can lead to temporary or permanent weakness. Post-surgical swelling or inflammation: Following MVD, the surrounding tissues, including the facial nerve, can experience swelling or inflammation. This may temporarily impair the function of the facial nerve. Anatomical variations: Variations in the anatomy of the vascular structures or the proximity of the facial nerve can increase the likelihood of facial nerve involvement during decompression. The management of post-operative facial paralysis typically involves a thorough evaluation to determine whether the condition is transient (due to inflammation or mild injury) or more persistent, which might require further intervention. Conservative treatments, such as corticosteroids or physical therapy, are often recommended for mild cases, while more severe or persistent cases might necessitate additional surgical approaches.
},
year = {2025}
}
TY - JOUR
T1 - Rare Complication of Microvascular Decompression: Delayed Facial Paralysis
AU - Preeti Singh
AU - Harsh Patel
AU - Abhaya Kumar
Y1 - 2025/08/20
PY - 2025
N1 - https://doi.org/10.11648/j.ijcts.20251104.11
DO - 10.11648/j.ijcts.20251104.11
T2 - International Journal of Cardiovascular and Thoracic Surgery
JF - International Journal of Cardiovascular and Thoracic Surgery
JO - International Journal of Cardiovascular and Thoracic Surgery
SP - 41
EP - 44
PB - Science Publishing Group
SN - 2575-4882
UR - https://doi.org/10.11648/j.ijcts.20251104.11
AB - Microvascular decompression (MVD) is a surgical procedure for relieving pressure on the trigeminal nerve caused by offending blood vessel, done by placing cushion between the two and is considered highly effective treatment for trigeminal neuralgia (TN). DFP refer to the facial paralysis which occurs more than 24 hours after MVD procedure and it can generally recover spontaneously. It common in clinical observation and its mechanism is still unclear. Facial paralysis can result from several mechanisms which includes inadvertent injury to the facial nerve as during the MVD surgery, the facial nerve, which lies in close proximity to the trigeminal nerve, can be at risk. Even a small amount of trauma to the facial nerve can lead to temporary or permanent weakness. Post-surgical swelling or inflammation: Following MVD, the surrounding tissues, including the facial nerve, can experience swelling or inflammation. This may temporarily impair the function of the facial nerve. Anatomical variations: Variations in the anatomy of the vascular structures or the proximity of the facial nerve can increase the likelihood of facial nerve involvement during decompression. The management of post-operative facial paralysis typically involves a thorough evaluation to determine whether the condition is transient (due to inflammation or mild injury) or more persistent, which might require further intervention. Conservative treatments, such as corticosteroids or physical therapy, are often recommended for mild cases, while more severe or persistent cases might necessitate additional surgical approaches.
VL - 11
IS - 4
ER -